
Sinus Surgery Set
The paranasal sinuses are air-containing cavities in certain bones of the skull that have openings to the nasal cavity. There are several paired paranasal sinuses, including the frontal, ethmoidal, maxillary and sphenoidal sinuses. The ethmoidal sinuses are further subdivided into anterior and posterior ethmoid sinuses, the division of which is defined as the basal lamella of the middle turbinate.
Acute sinusitis is usually the result of an earlier upper respiratory viral infection, but can also be due to fungal invasion. These attacks can be aggravated in cases of low immunity. Sinus surgery is needed in chronic bacterial sinusitis unresponsive to adequate medical treatment, as well as cases of recurrent acute bacterial sinusitis. Chronic sinusitis means that the inflammation remains in the nose and sinuses and does not go away over time (usually for at least 3 months). They are also indicated for cases of diffuse nasal polyposis, fungal sinusitis, antrochoanal polyps, mucoceles of the frontoethmoid or sphenoid sinuses and removal of nasal foreign bodies.
Frontal sinusitis can cause pain or pressure above the eyes with a headache in the forehead. Among all of the paranasal sinuses, acute frontal sinus bacterial infections have grave intracranial complications. The external approach of frontal sinus surgery is performed to prevent potentially life-threatening complications when the infection is unresponsive to maximal medical therapy or endoscopic sinus surgery. Mucoceles, extensive tumors, and trauma have also been identified as relative risk factors for endoscopic failure with conversion to the external approach. External frontoethmoidectomy can be used for the treatment of acute sinus disease with frontal extension.
Ethmoidal sinusitis can cause pain between the eyes and on the sides of the upper part of the nose. Refractory cases of ethmoid sinusitis are treated with intranasal or external ethmooidectomy.
Sphenoidal sinusitis can cause pain or pressure behind the eyes, but often refers to the top of the head. Chronic sphenoiditis is treated with sphenoidotomy, where access to the sphenoid sinus can be obtained by removal of its anterior wall.
Maxillary sinusitis can cause pain or pressure in the cheek area, as toothache, or headache. There are several documented external approaches for the treatment of chronic maxillary sinusitis. These include the antral lavage, which involves puncturing the medial wall of the maxillary sinus in the region of the inferior meatus and irrigating the cavity. This is indicated in chronic and subacute maxillary sinusitis, but not in acute maxillary sinusitis for fear of osteomyelitis. The thin lateral wall of the inferior meatus is punctured with a trocar and cannula, which are directed towards the ipsilateral ear.
Then, the trocar is removed and the cannula is advanced until it reaches the opposite antral wall. The antrum is then irrigated with a syringe until the wash is clear. Another operation was intranasal inferior meatal antrostomy, in which an opening is made in the nasoantral wall of the inferior meatus by an intranasal route. This operation is now rarely required and has been superseded by functional endoscopic sinus surgery. The Caldwell–Luc operation is a process of opening the maxillary antrum by a sublabial approach and dealing with the pathology inside the antrum. It is also called an anterior antrostomy as access to maxillary sinus is made through the anterior wall of the sinus. An incision cuts through the mucous membrane and periosteum, and a mucoperiosteal flap is raised until the infraorbital nerve to avoid injury of the nerve.
Using cutting burr or gouge and hammer, a hole is made in the antrum. The opening is enlarged using a Kerrison’s punch. Once the maxillary antrum has been opened, the pathology is removed. Diseased antral mucosa can be removed with elevators, curettes and forceps. This includes cysts, benign tumours, foreign bodies or polyps. A curved haemostat is pushed into the antrum from the inferior meatus and then this opening is enlarged with Kerrison’s forceps and side-biting forceps to make a window. The antrum is then packed and the wound is closed.
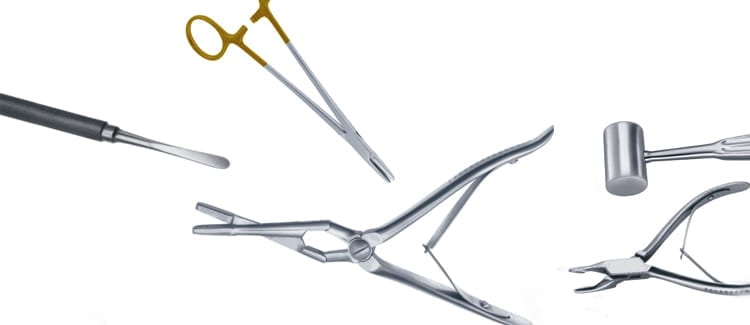
These procedures require a range of instruments to assist in manipulating and dissecting bony surfaces. Surtex instruments provides heavy-duty instruments for this purpose, such as the Molt Periosteal Raspatory / Elevator, the Blumenthal Bone Rongeur, the Miller-Colburn Bone File, and the Gerzog Bone Mallet.
Another important instrument we provide is the straight Cottle Osteotome is used for dividing and cutting deeply into bones in a straight manner, and are used by otolaryngologists for external osteotomy in rhinoplasty and for bone cuts in maxillectomy and mandibulectomy. The Cleveland Bone Cutting Forcep have precise and sharp jaws that make them useful in a variety of orthopedic or ENT procedures for cutting bone, with enhanced access to narrow surgical fields. The Fergusson Suction Tube can be used in cleaning procedures to remove blood or irrigation fluids, and assists in keeping the surgical field clean and visible.
A maxillary sinus floor augmentation increases the amount of bone in the posterior maxilla by lifting the lower Schneiderian membrane and placing a bone graft. We manufacture a range of Tatum Sinus Lift Curettes for this surgery. This is a double-ended device that consists of a central cylindrical handle which has two dissimilar curved tips on either side, in order to accommodate and conform to the different anatomical configurations that may be met in maxillary sinus procedures.
Join our newsletter
Specify the advantages, benefits of joining the newsletter, setting the spam rate.
Popular tags
Recent News
-

The Role of Vascular Clamps and Satinsky Clamps in Cardiovascular Surgeries
Cardiovascular surgeries are intricate procedures that demand the highest level...
-

The Essential Tools for Gynecological Procedures
The practice of gynecology necessitates a comprehensive set of specialized...
-

Orthopedic Surgery Essentials
Orthopedic surgery is a complex and highly specialized field requiring...
-

Mastering the Art of Ophthalmic Surgery
Ophthalmic surgery is a highly specialized field requiring precision, skill,...